

In clinical practice, the diagnosis of “Achilles tendinosis” is frequently encountered. However, what are the implications when such a diagnosis proves detrimental to a patient’s mobility?
I recently evaluated a patient whose case exemplified the critical “red flags” that specialists must recognise. After two decades of steroid therapy for polymyalgia rheumatica, the patient presented with a rupture of the left Achilles tendon, which was initially misdiagnosed by two previous clinicians as a non-rupture. Both clinicians failed to assess for, or diagnose the rupture and offered months of rehab for Achilles tendinitis.
The clinical red flag: Steroid-induced tendinopathy
Prolonged corticosteroid use is a well-documented cause of biomechanical disruption, compromising connective tissue integrity and significantly increasing the risk of “spontaneous” rupture. In this instance, the absence of a palpable tendon and the inability to perform a single-leg heel raise were definitive indicators that the condition labelled as “tendonitis” was, in fact, a complete structural failure. Long-term corticosteroid use has profound implications for the biomechanical integrity of the Achilles tendon, often predisposing it to degenerative changes and rupture. Corticosteroids inhibit the production of extracellular matrix collagen and impair local vascularisation, thereby initiating a degenerative cascade within the tendon tissue. This deterioration can lead to partial or complete tendon ruptures, sometimes presenting as seemingly “spontaneous” injuries without overt trauma. Misdiagnosis of such ruptures as mere tendonitis can delay appropriate treatment and contribute to a permanent decline in mobility and gait function (Vallone & Vittorio, 2014).
The biomechanical domino effect
Complicating this case further was the presence of an underlying anatomical leg length discrepancy (A-LLD).
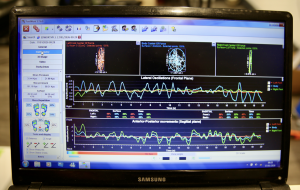
- My pressure plate analysis revealed increased heel pressure on the left side, with ankle instability in both feet during stance.
- Centre of mass (CoM) shift in stance and gait. The static stance was erratic, with the body searching for a stable foundation that was no longer available in the left posterior chain.
- “Pull” vs. “Push”: Gait analysis indicated an inefficient “push-off” (heel-lift) phase. As the Achilles tendon was unable to provide the necessary lever during the heel lift, the patient effectively pulled the heel at terminal contact, ‘dragging’ the limb through space. The gait was so unstable that a fall-risk was high.
- Adaptation at pelvic level to the A-LLD with a posterior innominate rotation (PI ilium) on the longer limb side and anterior innominate rotation (AS ilium) to the shorter limb side.
Effective and simple solution
Rather than resorting to invasive surgery or a cumbersome Richie brace, we implemented a simple targeted mechanical strategy.
- Stability via a full length OTC ankle-foot orthoses (AFO).
- Addressing the LLD: A 5–6 mm heel raise on the right (shorter) side limb balanced the pelvis and reducing adaptation. This has the effect of stabilising the CoM providing increased confidence during gait.
- Neuromuscular re-education in the form of gait training. This can be quite simple by advising the patient to:
- Encourage “rolling” the foot heel-to-toe”
- Increasing arm swing to drive momentum, essentially utilising the upper body to assist the compromised lower body levers. Enhanced arm swing and increased cadence can help stabilise the CoM and reduce medio-lateral sway.
- Lifting the head and walk more upright.
- Encourage a purposeful gait to increase confidence.
- Advice the use to running shoe. In this case Brooks.
Rehabilitation strategies that extend beyond mechanical correction are imperative. Neuro-muscular re-education protocols focusing on restoring coordinated movement patterns such as promoting a heel-to-toe rolling gait and enhancing arm swing to augment momentum have demonstrated benefits in stabilizing the CoM and reducing medio-lateral sway. These rehabilitation principles leverage the kinetic contribution of the upper body to compensate for plantarflexor deficits, enhancing overall gait efficiency and decreasing fall risk (Baxter et al., 2018)
A small fragment of the ruptured Achilles had naturally reformed, however following the rupture, the biomechanical consequences extend beyond the tendon itself to affect the related musculature and gait mechanics. Post-rupture remodelling of the gastrocnemius muscle, characterised by decreased muscle thickness and altered fibre architecture, compromises the ability of the plantar flexor unit to generate sufficient work and power during activities such as single-leg heel raises, which are critical for normal walking propulsion (Baxter et al., 2018). The inability to perform an effective “push-off” phase results in compensatory gait patterns, such as an ineffective “pull” of the foot during terminal contact, which further destabilises the CoM and compromises the overall balance and mobility.
The takeaway for practitioners
Complex cases of Achilles tendon rupture frequently co-occur with structural biomechanical imbalances, including leg-length discrepancies (LLD). Untreated LLD can lead to asymmetric loading and uneven force distribution across the lower limbs, exacerbating tendon stress and impairing stability. Although the literature does not provide direct studies on LLD correction in this context, clinical practice supports the use of targeted interventions, such as heel lifts on the shorter limb, to restore pelvic and lower limb symmetry, which, in turn, reduces aberrant loading patterns on the injured side. Additionally, AFOs particularly full-length models that stabilise the subtalar joint without overly restricting motion, have proven effective in providing immediate mechanical support and leverage to the ankle. These devices aid in controlling excessive joint motion, thereby supporting tendon healing and improving functional gait dynamics.
Failure to consider both systemic history (steroids) and structural imbalances (A-LLD) results in an incomplete clinical picture. Misdiagnosing a rupture as tendonitis not only delays healing but also permanently alters the patient’s gait and quality of life. Approaching complex cases from a straightforward perspective is recommended.
The patient was not seeking complex and costly long-term rehabilitation but simply desired to navigate her home and community without the risk of falling. To this end, I stabilised her CoM with an inexpensive heel lift for the shorter limb and improved her gait with a full length inexpensive OTC AFO to assist with the delayed heel lift on the longer, ruptured side. This simple and moderate solution cost the patient no more that £50, however the value to her existence was priceless. The smile on her face says it all. With consent to post.
References
Baxter, J. R., Hullfish, T. J., & Chao, W. (2018). Functional deficits may be explained by plantarflexor remodeling following Achilles tendon rupture repair: Preliminary findings. Journal of Biomechanics, 79, 238–242. https://doi.org/10.1016/j.jbiomech.2018.08.016
Vallone, G., & Vittorio, T. (2014). Complete Achilles tendon rupture after local infiltration of corticosteroids in the treatment of deep retrocalcaneal bursitis. Journal of Ultrasound, 17(2), 165–167. https://doi.org/10.1007/s40477-014-0066-9

Left partially attached Achilles

Left Achilles rupture
Left ankle unstable during stance
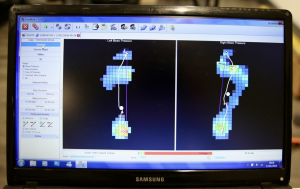
CoM displaced right